March exam
https://medicinedepartment.blogspot.com/2021/03/medicine-paper-for-march-2021-bimonthly.html?m=1
Answer all questions
Max Marks: 100 (10 marks for each answer) .
1) Please go through the patient data in the links below and answer the following questions:
https://ashakiran923.blogspot.com/2021/03/60-years-old-male-fever-under-evaluation.html?m=1
a). What is the problem representation of this patient and what is the anatomical localization for his current problem based on the clinical findings?How specific is his dilated superficial Abdominal vein in making diagnosis?
A) 60 yr old male with complaints of fever and sob
Pt is having ascitis and splenomegaly which indicates portal htn ( Hepatic cause of portal hypertension probably micro nodular cirrhosis ) ,as there is gross ascitis and mild splenomegaly .
Fever and Sob can be due to underlying pneumonia of left lower lobe .( Cxr picture isn't available here).
Pt also has AKI on CKD ( due to gross ascitis and third space loss - pre renal aki ) .
Dilated superficial abdominal veins indicate portal hypertension , flow away from umbilicus indicate cirrhosis and flow towards umbilicus indicate post hepatic portal htn - IVC obstruction etc
b) What is the etiology of the current problem and how would you as a member of the treating team arrive at a diagnosis? What is the cause of his hypoalbuminemia?Why is the SAAG low?
A) Etiology of his current problem is portal hypertension and sepsis
Micronodular cirrhosis causing hypoalbunemia .
Saag is low as pt is also having ckd and losing protein in urine . A 24 hr spot protein creat ratio would help in diagnosis.
c)Will PT,INR derangement preceed hypoalbuminemia in liver dysfunction??Share reference articles if any!
A) Pt inr will be affected first in liver dysfunction after that albumin will be decreased ,as half life of albumin is 3 weeks .
d)What is the etiology of his fever and pancytopenia?
A) Pancytopenia secondary to hypersplenism.
QUESTION 2
45year old female with abdominal distension
https://navyamallempalli.blogspot.com/2021/02/dr_6.html
a). What is the problem representation of this patient and what is the anatomical localization for her current problem based on the clinical findings?
A ) 45 yr old female with abdominal distension and pedal edema - problem representation and localisation :
- Gross ascitis
Right massive pleural effusion with collapse
High saag and low protein - indicating portal hypertension probably secondary to chronic Budd Chiari syndrome or liver metastasis.
So pt developed gross ascitis secondary to portal hypertension ( chronic Budd Chiari syndrome ) / liver metastasis.
Primary could be breast ,lung ,colon ,stomach ,esophagus.
Right massive pleural effusion was transudative on examination , probably Hepatic hydrothorax.
Hepatic hydrothorax (HH) is the excessive (> 500 mL) accumulation of transudate in the pleural cavity in patients with decompensated liver cirrhosis (LC) but without cardiopulmonary and pleural diseases. Its localization is right-sided in approximately 85% of cases and left-sided in approximately 13%; whereas, only 2% of patients have fluid in the pleural cavity on both sides.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5680207/#!po=7.29167
b) What is the Etiology of her refractory ascites and pleural effusion? and how would you as a member of the treating team arrive at a diagnosis?
A) Refractory ascitis is secondary to malignancy and hypoalbunemia.
c) Approach to a patient with ascites?Clinically is there any way to differentiate pre hepatic, post hepatic and hepatic causes?
A)



Clinically pre hepatic portal htn have massive splenomegaly and minimal ascitis . On usg there will be portal cavernoma if there is portal vein obstruction.
Hepatic cause of portal hypertension will have shrunken liver ,derranged coagulation profile, bleeding manifestations ,jaundice ,pedal edema ,ascitis due to hypoalbunemia . In micronodular cirrhosis liver echotexture can be normal.
Post hepatic cause of portal hypertension can also have ascitis , splenomegaly but raised jvp can be present clinically if there is constrictive pericarditis or CCF / IVC obstruction.
d)Causes of budd chiari syndrome?Why did the patient undergo bone biopsy?
A)

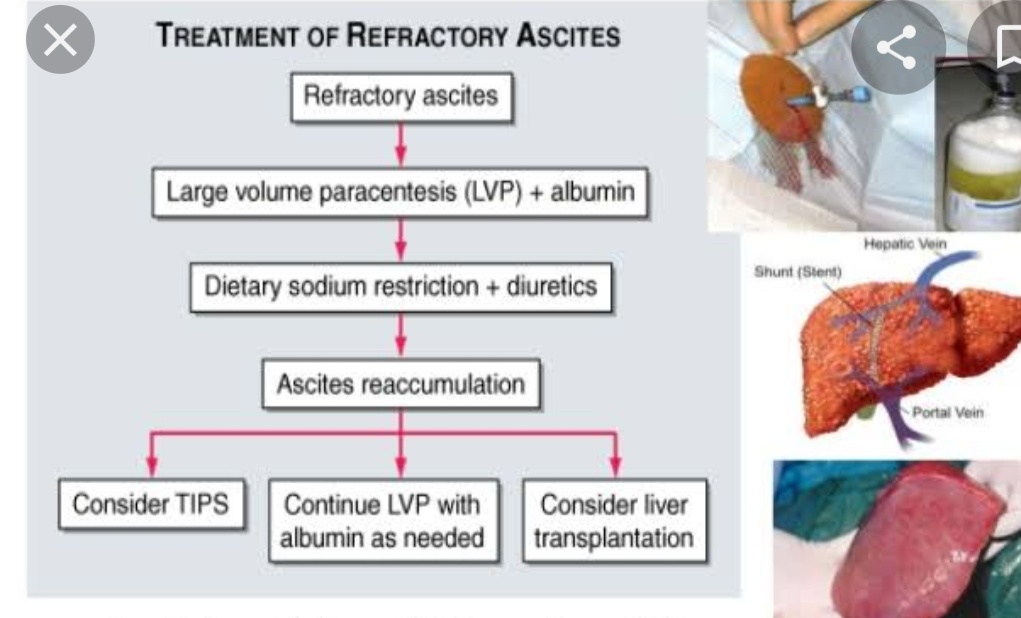
d) Management strategies for refractory ascites and Budd chiari syndrome? Share the potential advantages and disadvantages of Peritoneal dialysis catheter placement in refractory ascites?
A)

4 ) What is the efficacy of each of the drugs listed in his current treatment plan ?
Therapy of varices and variceal hemorrhage in the adult patient with cirrhosis needs to be stratified depending on the different clinical stages in the natural history of portal hypertension: (1) the patient with cirrhosis and portal hypertension who has not yet developed varices and in whom the goal is to prevent the formation of varices (pre-primary prophylaxis); (2) the patient with gastroesophageal varices who has never had bleeding from them, and in whom the goal is to prevent their rupture (primary prophylaxis); (3) the patient with acute variceal hemorrhage in whom the goal is to stop the hemorrhage and prevent its early recurrence; and (4) the patient who has survived an episode of acute variceal hemorrhage, in whom the goal of therapy is to prevent late recurrence of hemorrhage (secondary prophylaxis).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3309905/#!po=45.2381
QUESTION 3
55year old male with SOB and abdominal distension,orthopnea
https://jayanth1802.blogspot.com/2021/02/55-year-old-farmer-with-sob-abdominal.html?m=1
a). What is the problem representation of this patient and what is the anatomical localization for his current problem based on the clinical findings?
A) 55 yr old male with complaints of sob and generalised anasarca .
Problem representation and anatomical localisation :
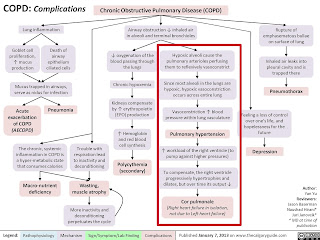
- Pt is a chronic smoker and has copd causing pulmonary artery hypertension and thereby cor pulmonale ( Right heart failure ) .
Right heart failure leading to gross ascitis and pedal edema due to increased hydrostatic pressure.Pt is also having high saag indicating portal hypertension - post hepatic cause of portal hypertension.
Pt is having bicytopenia which can be secondary to vit b12 deficiency or ? Hypersplenism secondary to portal hypertension but there is no evident splenomegaly.
b) What is the etiology of his ascites? and how would you as a member of the treating team arrive at a diagnosis?Chart out the sequence of events!
A) Pt is having ascitis secondary to portal hypertension ( post hepatic cause ) . Diagnosis can be confirmed by ascitic fluid therapeutic tapping which is showing saag - 1.9 ( high saag indicative of portal htn ) .
Sequence of events :
Chronic smoking - COPD and PAH --- right heart failure -- post hepatic portal hypertension ---ascitis--third space loss and causing AKI ( pre renal ) --metabolic acidosis .
4)Please go through the thesis presentation below and answer the questions below by also discussing them with the presenter.
a)What was the research question in the above thesis presentation?
To know the etiology of ascitis based on SAAG
b) What was the researcher's hypothesis?
SAAG is better for etiological diagnosis of asctis than asctic fluid total protein as a marker
c)What is the current available sensitivity and specificity of SAAG in diagnosis of etiology of ascites
The sensitivity and specificity of SAAG were 100% and 87.8% respectively. Serum ascites albumin gradient is a reliable marker to differentiate ascites into portal hypertensive and non-portal hypertensive etiology. the presence of oesophageal varices is significantly associated with high SAAG levels.
5) Journal club questions on Ascites theme
a) Please identify the study design and outcomes in the article linked here https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6644216/ as well as the thesis linked here https://chandanavishwanatham19.blogspot.com/2021/03/of-thesis-clinical-profileevaluationdia.html
The study design was a prospective study and it showed that liver cirrhosis is the main cause of ascites among the 52 patiens included in the study and next most common cause being heart failure and nephrotic syndrome.
And the etiology of liver cirrhosis being HCV HBV virus.
B)
) Please download the CASP diagnostic study checklist here
https://casp-uk.net/casp-tools-checklists/ to evaluate the paper here https://www.hindawi.com/journals/ijh/2019/8546010/ and share your learning points on critical appraisal of the paper.

Comments
Post a Comment