42year male with Alcohol liver disease,Hypertriglyceridemia
CHEIF COMPLAINTS
42year male Supervisor in petrol bunk came with c/o (on 24-4-2023)
1)Vomiting - 3episodes in the night(8pm on 23-4-2023)
2)Pain abdomen-Diffuse(in the morning 4am)
HISTORY OF PRESENTING COMPLAINTS
He studied till intermediate,later he left his studies and entered in to family finance business later wine shop business.He started drinking beer, toddy from year 2000 (occasionally during gatherings------>weekly once------->daily(1beer/day).
He lost his mother in 1994(his age-13yr),She struggled for 8months with cancer.His father also drinks alcohol around 90-180ml/day,had a CVA(Right hemiplegia) in 2007---->bed ridden for 2years--->died in 2009.He had a elder brother, who went to Bombay,also died due to excess alcohol consumption(?Liver cirrhosis)
He got married in 2004(age-21yr).From 2015 patient started taking beverages with high alcohol content,due to stress from his business loss.From 2020 he gave up all his own business and started working as an employee in petrol bunk as supervisor
In 2020 when he was returning from a function(under alcohol influence) had an RTA(skid from bike),brought to hospital Intermedullary nailing was done to his right femer.He was diagnosed as Diabetic and hypertensive during the event
Patient takes 90ml/day IB brand liquor.on 23-4-2023 at 8pm patient had vomiting 3 episodes non bilious, non projectile, contains food particles,non foul smelling,non blood tinged.Associated with diffuse abdominal pain, not relieving on bending forward.As the intensity of pain increased in the morning, he came to our causality at 4am
No history of any fever,loose stools,chest pain, palpitation,cough,constipation,obstipation
PAST HISTORY
K/C/O DM2(on metformin 500mg) & HTN(On Amlodipine 5mg).
PERSONAL HISTORY
Mixed diet
Regular bowel and bladder habits
Alcoholic since 23years(takes 90ml/day -IB brand liquor)
Daily routine : wakes at 8:00am,bathe and eat tiffin,9am goes to petrol bunk.supervises the bill collections till 6:00pm and return home with 90ml IB brand liquor.Drinks at 8:00pm,Eat dinner at 9:30pm and goes to sleep by 10:00pm
FAMILY HISTORY
Mother expired due to cancer and Father expired Post CVA sequle.Brother expired bcz of ?liver cirrhosis
MEDICAL HISTORY
Tab Metformin 500mg once daily at 8:00am
Tab Amlodipine 5mg once daily at 8:00am
GENERAL EXAMINATION
Patient is conscious, coherent,co-operative.Moderately built and Moderately nourished.
Blood pressure-130/70mmhg,right arm, supine position
Pulse-90/min,regular rythm,normal volume.
Respiratory rate-20/min,thoraco abdominal
Temperature-98 F
Spo2-98% on room air
Grbs-175mg/dl
Icterus+
No pallor,clubbing,cyanosis,lymphedenopathy,edema of legs
No raised JVP





SYSTEMIC EXAMINATION
CARDIOVASCULAR SYSTEM :
-Elliptical & bilaterally symmetrical chest
-No visible pulsations/engorged veins on the chest
-Apex beat seen in 5th intercostal space medial to mid clavicular line
-S1 S2 heard
-No murmurs
RESPIRATORY SYSTEM
Upper respiratory tract normal
Lower respiratory tract :
-Trachea is central
-Movements are equal on both sides
-On percussion resonant on all areas
-Bilateral air entry equal
-Normal vesicular breath sounds heard
-No added sounds
-Vocal resonance equal on both sides in all areas
CENTRAL NERVOUS SYSTEM :
-Higher mental functions intact
-Cranial nerves - intact
-Sensory system-normal
-Motor system -normal
PER ABDOMEN



-Scaphoid
-No visible pulsations/engorged veins/sinuses
-Soft,non tender, no guarding and rigidity,organomegaly +(Liverspan-18cm)
-Bowel sounds heard
PROVISIONAL DIAGNOSIS
Pain abdomen secondary to ?Alcoholic bowel dysfunction ?Acute Pancreatitis ?Acute cholecystitis
k/c/o DM2 & HTN(since 2years)
INVESTIGATIONS












Serology-Negative


FINAL DIAGNOSIS
Alcoholic liver disease,Hyper triglyceridemia,Thrombocytopenia
K/C/O DM2 & HTN (2years)
--------------------------
BILIRUBIN ANALYSIS IN OUR LAB--Modified JENDRASSIK & GROF'S METHOD
After receiving blood in red vacutainer,it is centrifuged

Serum obtained is mixed with reagent Diazo reagent


After mixing the serum with reagents,Test tube are kept in BS-390 analyser(Most of the biochemical tests can be done in this machine)




Sample process time=30min,
other tests done in this BS-390

If the sample is showing high bilirubin value then technician re-confirm with BA100 machine




-------------------------------------------------------------------------------------------------
Discussion around the case
PROFESSOR:
What is the link between alcohol and hypertryglyceridemia?
What are the clinical examination findings in familial hypertryglyceridemia and does your patient have any of these findings?
What is the sensitivity specificity of clinical findings v family history v genomic studies in the diagnosis of familial hypertryglyceridemia?
Student :
https://pubmed.ncbi.nlm.nih.gov/21245063/
Aims: This study was conducted to examine the relationship between triglyceride (TG) levels and a history of excessive drinking in patients with severe hypertriglyceridemia (HT)
The study included 300 patients with TG levels ≥ 11.3 mmol/ l (1000mg/dl), 220 men and 80 women
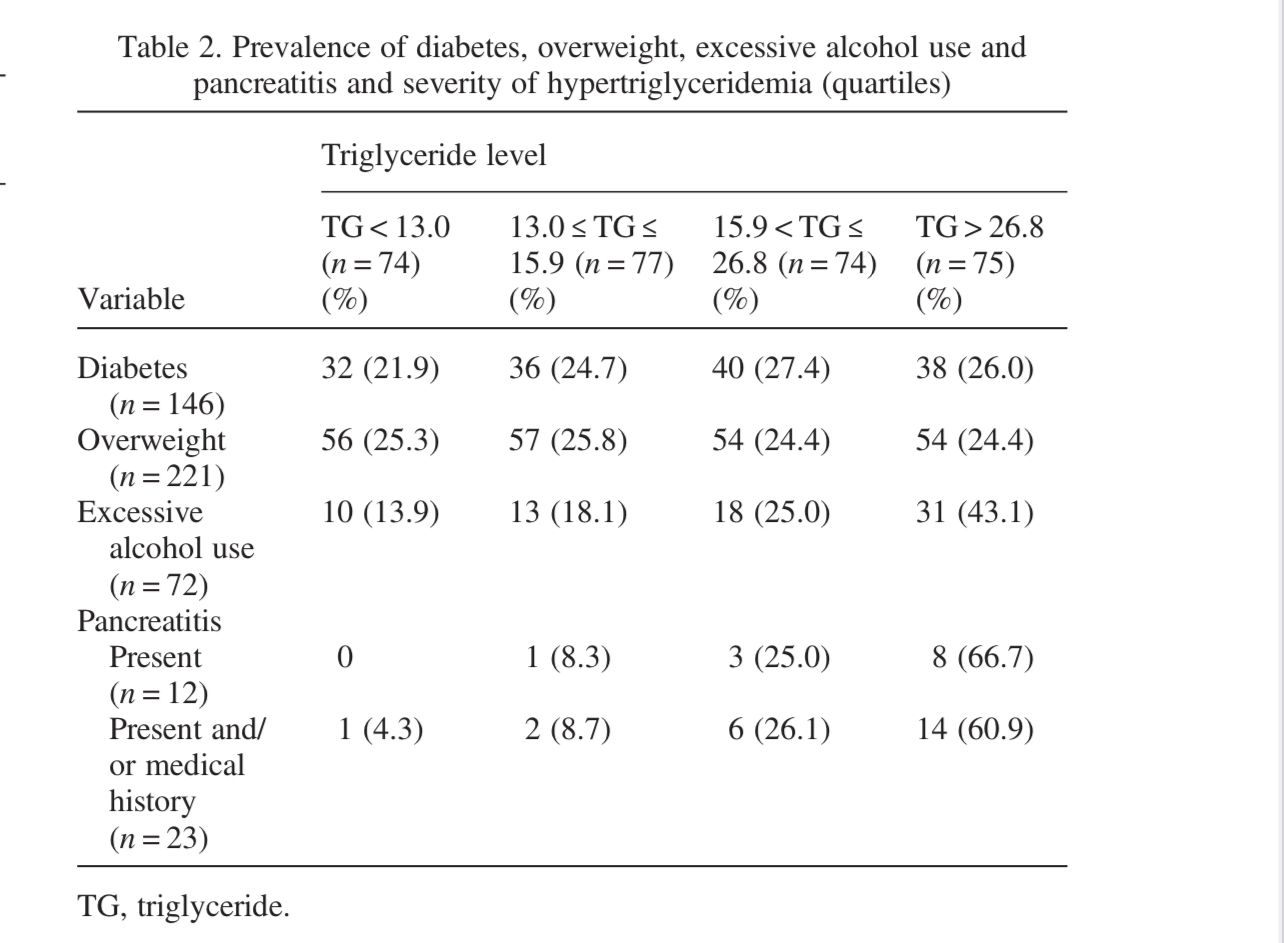
Among 72 patients of excess alcohol 🍺 intake(among 300)
TG levelMmol/L. Mg/dl. n=72
<13. <1150. 10
13–16. 1150–1400. 13
16-27. 1400-2370. 18
>27. >2370. 31
PROFESSOR : What are the learning outcomes here in the context of improving this patient's illness outcomes?
STUDENT : There is a direct co-relation between alcohol intake & increasing triglyceride level

Have shown these numbers to him & Advised for DAC admission sir
Explained about adverse effect of his 20years of alcohol consumption & risk of further liver cirrhosis,Acute pancreatitis,Coronary artery disease
STUDENT :
Regarding familial hypertriglyceridemia
On clinical examination
1)Eruptive Cutaneous xanthomas
2)Tuberous xanthomas
3)Palmar crease xanthoma
Are not seen sir
Case report showing manifestation of familial hypertriglyceredemia.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1839776/

STUDENT :
Sir,
I couldn’t find exact values of sensitivity & specificity of
1)Clinical findings
2)Family history
3)Genomic studies
In diagnosing Familial Hypertriglyceridemia
But i could find a paper on “FCS score “ sensitivity & specificity * the overall sensitivity of the FCS score (≥10) was 88% with an overall specificity of 85% *(https://pubmed.ncbi.nlm.nih.gov/29980054/)


Comments
Post a Comment